Soft Silicone Adhesives Crucial for Atraumatic Advanced Wound Care Dressings
Silicone adhesive dressings minimize pain, promote wound healing, and improve clinical and financial outcomes for caregivers.


Mention the words “silicone” and “medical” in the same sentence, and it’s arguable that most people will immediately think of silicone’s well-known (and occasionally maligned) usage in artificial breast implants. However, silicone has other significant and successful applications in medical products.
Silicone is particularly successful as an adhesive for advanced wound care dressings, which has been one of the most challenging riddles in dressing manufacturing and usage for nearly half a century. In recent years, silicone dressings have blossomed into a segment that garners $130 million annually; these figures are projected to increase.
Advanced Wound Care
Advanced wound care (AWC) is a collection of therapies for difficult-to-treat or chronic wounds, such as amputations, diabetic foot ulcers and pressure ulcers (bedsores), which cannot heal with standard dressings. AWC dressings are made from a host of materials, including foams, alginates, hydrocolloids, gels and even honey.
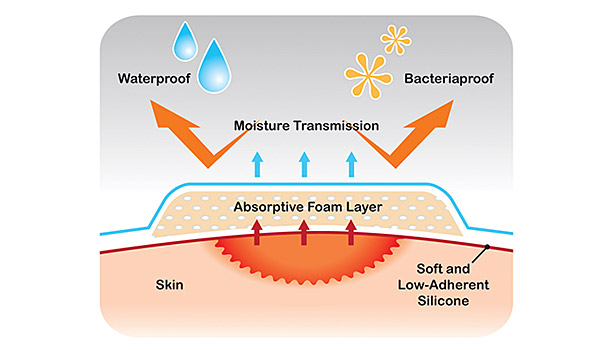
AWC often relies on therapies (better known as interventions) that promote a moist wound healing (MWH) environment. This is quite different than the more common “keep it dry and clean” practices used with Band-Aids® to treat minor wounds at home, or gauze-and-sterile-tape dressings for wounds severe enough to require an emergency room visit.
Despite the differences, simple dressings such as bandages or gauze-and-tape share two fundamental similarities with AWC dressings. First, all need to protect a wound from infection, promote its healing and stay adhered. Second, sooner or later, they all need to be removed or changed. That notion about adhesion—whether it’s a simple bandage or an advanced wound care dressing—is a challenge for manufacturers and caregivers, both to ensure adhesion while a dressing is worn and to minimize pain and damage when it’s removed.
Most people can relate to the sting of removing a bandage or tape for a relatively minor wound. Fortunately, fewer can relate to the unspeakable pain of removing a dressing from a severe ulcer or amputation, especially if it is made with more common (and less expensive) polyacrylate adhesives. In addition, wounds that can be treated with bandages or gauze-and-tape typically heal in a matter of days or weeks. Wounds that require MWH often require months—and sometimes up to a year—to heal. That’s a lot of dressing changes and, consequently, a lot of pain, which is only part of the problem.
As with any wound, the skin and tissue surrounding it are delicate and volatile. This is especially true for wounds that require MWH, which promotes maceration, or the softening and breaking down of skin after prolonged exposure to moisture (especially after several weeks or months). Coupled with the repeated application and removal of tacky adhesive dressings during MWH that often prolong the healing process, a demand was created for alternative adhesives.
The Silicone Adhesive Solution
By the end of the 1980s, wound care dressing manufacturers had started to innovate soft silicone dressings that not only fostered wound healing, but were atraumatic, meaning that they were both non-adherent to the wound bed and low-adhesive to the skin. However, in the 1990s, two crucial aspects soon hindered that innovation and mainstream adoption. The first was related to massive litigation against silicone breast implant producers, which somewhat discouraged silicone dressing applications involving open wounds. The second complication occurred later in the decade, when manufacturers resumed innovation and began to master soft silicones’ low-tack adhesive properties; their relatively high price marginalized them as a “premium dressing,” which limited their use.
That landscape has very recently started to change, in no small part due to the Affordable Care Act. Hospitals, clinics, long-term care facilities and home health agencies’ reimbursements are increasingly determined by clinical outcomes, which have impacted the perceived economic value of silicone dressings. Rather than using less expensive alternatives that may yield less optimal results, silicones are emerging as an ideal dressing—both clinically and financially speaking. The importance of balancing clinical outcomes and the cost of care are now at the forefront in the restructuring of the U.S. healthcare model.
This has motivated smaller companies to produce soft-silicone dressings that are as efficient but more competitively priced than those offered by large companies that currently own the lion’s share of silicone dressing sales. The new paradigm is poised to be a win-win-win for all: manufacturers, caregivers and, most importantly, advanced wound care patients who can pay less for reduced pain and better outcomes—all thanks to silicone adhesives.
For more information, visit www.medipurpose.com/mediplus.
Looking for a reprint of this article?
From high-res PDFs to custom plaques, order your copy today!